
ROLE OF CT SCAN IN DIAGNOSIS OF INFLAMMATORY RENAL DISEASES
1Aadil Hussain Dar*, 2Ashita Jain, 2Navreet Boora, 3Aqib Rashid Parray
1Assistant Professor, Faculty of Allied Health Sciences, Bhai Gurdas group of institutions, Sangrur, Punjab, India
2Assistant Professor, Department of Paramedical Science, Faculty of Allied Health Science, SGT University India
3Assistant Professor, Department of Allied Health Science, Brainware University, Kolkata (WB) India
DOI: https://doi.org/10.62502/ijmi/tyxpxs95
ABSTRACT
Background: Inflammatory renal diseases encompass a diverse group of conditions characterized by kidney inflammation, leading to varying levels of renal impairment and structural damage. Computed tomography (CT) has become an indispensable tool for evaluating these conditions, providing detailed insights into anatomical and functional abnormalities. Aim and Objectives: The study aims to evaluate hydronephrosis and other renal diseases using CT imaging to understand its diagnostic utility in inflammatory renal conditions. Methodology: A cross-sectional analysis was conducted, utilizing CT scans from a minimum of 80 patients, including both males and females. Results and Conclusion: CT imaging proved to be a valuable modality for detecting and characterizing inflammatory renal diseases. Its ability to identify both anatomical and functional abnormalities underscores its significance in modern renal disease diagnosis and management.
Keywords: Computed Tomography, Chronic Kidney Diseases, Renal Inflammation
INTRODUCTION
The kidneys are essential for maintaining homeostasis, or internal balance, as well as for controlling blood pressure, producing blood cells, balancing the acid-base system, excreting toxins and metabolic waste products, maintaining salt and water homeostasis, and regulating calcium (Ca2+) homeostasis. As a result, renal diseases are among the main reasons for morbidity, mortality, and medical expenses. The restricted traditional understanding of kidney function concentrates on controlling the excretory, endocrine, acid-base, and electrolyte domains [1]. Inflammatory renal diseases comprise a broad category of medical conditions that impact the kidneys and can be difficult to diagnose and treat. There are several causes of inflammation in the renal parenchyma, such as autoimmune disorders, infections, and systemic illness. These disorders can present with minor functional abnormalities in the kidneys or with significant damage to the parenchyma, abscess formation, and possibly fatal consequences. The variety of inflammatory renal diseases, which include conditions like renal abscesses, glomerulonephritis, and pyelonephritis, creates particular difficulties for clinical evaluation. The field of diagnostic radiology has been completely transformed by the revolutionary development of Computed Tomography (CT), also referred to as Computerized Axial Tomography (CAT) [2]. With the help of a CT scan, internal structures of the body can be visualized in three dimensions with minimal discomfort as they produce precise cross-sectional images of the human body. Since then, this imaging modality has grown to be an essential part of the healthcare system helping to diagnose, stage, and monitor a variety of illnesses. The basic idea behind CT imaging is to produce finely detailed cross-sectional images of the body using X-rays. In contrast to conventional X-rays, which yield two-dimensional images, a CT scan produces a sequence of thin, stacked slices known as "tomograms." These slices are subsequently processed by a computer to create intricate, high-resolution pictures that offer a thorough view of the targeted anatomy. CT scans play a vital role for doctors in a variety of medical specialties because they make soft tissues, bones, blood vessels, and organs remarkably clear, thus assisting them in the surgical field as well [3].
|
Corresponding Author: Mr. Aadil Hussain Dar, Assistant professor, Faculty of Allied Health Sciences, Bhai Gurdas group of institutions, Sangrur, Punjab, India |
Role of CT in Assessment of Inflammatory Renal Disease: For xanthogranulomatous pyelonephritis, computed tomography (CT) is the gold standard of diagnostic imaging because it provides a reliable diagnosis and details the extrarenal nature of the illness [7]. CT plays a significant role in the assessment of renal tuberculosis because it can accurately measure the proportion of remaining functional parenchyma, extra renal dissemination, and early symptoms such as papillary necrosis or calyceal erosion [9] After all, a CT scan is more sensitive and accurate in determining the specific position, size, degree, and extent of the loculation concerning other retroperitoneal structures, it is the preferred diagnostic method for evaluating perinephric abscess [4].
CT evaluation of severe renal inflammatory disease in children: Children with renal inflammatory disease are typically given a clinical diagnosis that is accurate and is promptly and successfully treated. But occasionally, there is either a murky diagnosis or a poor response to treatment. In these situations, a radiographic evaluation is necessary to determine the kind and severity of the patient's illness [10]. In the days before CT scanning, intravenous urography was typically used to examine these patients. However, prior studies have demonstrated that 72–75% of individuals with acute pyelonephritis had normal intravenous urography our experience has shown that information regarding the actual degree of renal and perirenal involvement is incomplete, even in cases where the intravenous urogram is aberrant. For these patients, a CT scan provides a more precise assessment [5].
The aim of this study is to assess the role of computed tomography (CT) in the diagnosis of inflammatory renal diseases. The objectives include evaluating hydronephrosis in the kidneys using CT imaging and analyzing various renal conditions to determine the effectiveness of CT as a diagnostic tool. This study seeks to highlight the significance of CT in identifying anatomical and functional abnormalities associated with renal diseases.
METHODS & MATERIAL
This prospective and cross-sectional study was conducted over two years (October 2022 to June 2024) in the Department of Radio-Diagnosis at SGT Medical College, Hospital & Research Institute, Gurugram, Haryana. The study included 80 patients, both male and female, of all age groups who were referred for CT imaging and diagnosed with inflammatory renal diseases. Data collection occurred between September 2023 and March 2024, focusing on CT imaging using the SIEMENS modality. Inclusion criteria encompassed all age groups and genders undergoing CT imaging for renal disease evaluation, while exclusion criteria included pregnant patients and those with contrast intolerance. Statistical analysis was performed using Microsoft Excel to calculate averages and other metrics.
RESULT
|
A large sample size was included in the study where the lowest age group was a 13-year patient and the highest age group was 88 years old comprising age groups of 12-91 yrs. in males and 4-76 yrs. in females (Table: 1). |
Table 5.1
|
Gender |
Age Group |
Average |
|
Male |
12-91 yrs. |
37.4 |
|
Female |
4-76 yrs. |
39.6 |
|
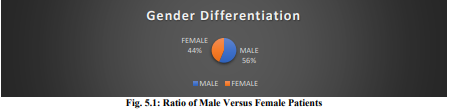
While categorizing the patients on the basis of their genders it was found out that, the proportion of female patients (n=35, 44%) was higher than that of male patients (n=45, 56%%). (Fig: 5.1) |
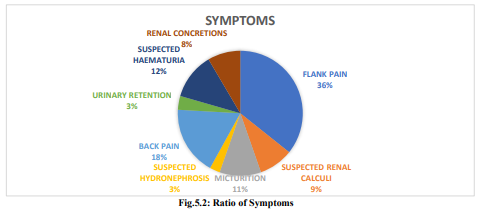
In our study, we categorized the patients according to various symptoms identified during the pre-assessment. We found that the majority had a history of flank pain (36%), followed by back pain (18%), suspected hematuria (12%), burning micturition (11%), suspected renal calculi (9%), and renal concretions (8%). Additionally, urinary retention and hydronephrosis were observed in 3% of the overall sample (Fig: 5. 2).
Another conclusion was drawn from the final observations detailed in the reports. It was noted that hydronephrosis had the most significant impact at 39.25%, followed by renal calculi at 22.43%, renal cysts at 15.89%, renal concretions at 13.08%, and other conditions making up approximately 9.35% (Fig. 5.3).

The study covered a wide age range, from 13 to 88 years, with the majority falling between 12 and 91 years for males and 4 to 76 years for females. Notably, females made up 44% of the sample, surpassing males at 56%. Patients were carefully categorized based on their pre-assessment symptoms, revealing that flank pain was the most common (36%), followed by back pain (18%), suspected hematuria (12%), burning sensation during urination (11%), suspected renal stones (9%), and renal concretions (8%). Additionally, urinary retention and hydronephrosis were each present in 3% of cases. The study's findings emphasized hydronephrosis as the most prevalent condition at 39.25%, followed by renal stones (22.43%), renal cysts (15.89%), renal concretions (13.08%), and other conditions (9.35%). These results highlight the varied symptomatic presentations and the significance of hydronephrosis as a notable concern among the study participants.
DISCUSSION
This study looks into how patients with renal inflammatory diseases might be evaluated using computed tomography. A notable finding in this research was the considerable occurrence of hydronephrosis, identified in 39.25% of the patients. Hydronephrosis, which occurs when the kidney swells due to an accumulation of urine, is frequently a complication arising from obstructive uropathy. The significant prevalence of this condition within the sample underscores the importance of prompt detection and treatment. Our study suggests that renal conditions are not restricted to a particular age range but impact people throughout various stages of life. The age distribution indicated that males predominantly experienced health issues between the ages of 12 and 91, whereas females exhibited renal problems from ages 4 to 76. While Mahmood et al. (2017) research emphasizes that younger patients primarily present with genetic renal disorders and glomerulonephritis. In contrast, older patients exhibit a higher occurrence of renovascular disease and hypertension, suggesting that different renal conditions within the chronic kidney disease population are more common in distinct age groups [6]. Our study found that flank pain was the most frequently reported symptom (36%), with back pain coming in second at 18%. While previous study by Bansal (2014) suggest that Patients experiencing sudden side pain show high levels of accuracy (97-100%) in sensitivity and (92-98%) in specificity when identifying kidney stones [8]. Other diagnoses encompassed renal cysts (15.89%) and renal concretions (13.08%). Renal cysts are frequently observed in imaging examinations and are typically asymptomatic; however, they have the potential to advance to more serious complications. The occurrence of renal concretions, although marginally less prevalent, may indicate the initial stages of stone formation or the presence of diminutive stone fragments. The residual 9.35% of diagnoses were attributed to various other renal disorders, indicating a heterogeneous spectrum of pathologies within the study cohort. In conclusion, this investigation illustrates a significant prevalence of hydronephrosis and renal calculi within the study cohort, accompanied by an array of additional renal conditions. The findings emphasize the necessity of contemplating a broad spectrum of symptoms and diagnoses when evaluating patients exhibiting renal complaints. In light of the observed gender and age distribution, subsequent studies should endeavor to further explore the specific risk factors pertaining to renal diseases across diverse demographic groups. Furthermore, proactive intervention strategies, particularly in relation to hydronephrosis and renal calculi, could potentially alleviate the progression of these conditions and enhance patient outcomes.
CONCLUSION
For complex disease courses and certain chronic inflammatory diseases, computed tomography has emerged as the preferred imaging modality in both adult and pediatric populations. Furthermore, CT is thought to be the best initial study to choose for a hospitalized patient with a suspected kidney illness. If an abscess is present, CT can also suggest the best moment to intervene; F.N.A.B. can be carried out with their assistance. A comprehensive approach is necessary for the precise diagnosis and efficient treatment of inflammatory kidney disorders. Healthcare practitioners can determine the underlying cause, severity, and extent of renal inflammation by using a comprehensive strategy that includes imaging scans, laboratory testing, physical examinations, and health histories.
REFERENCES
- (2012). E g atkinson, mbchb, msc, mrcp. British Journal of Ophthalmology, 75(11), 704–704. https://doi.org/10.1136/bjo.75.11.704-a
- Kawashima, A., et al. ‘CT of Renal Inflammatory Disease.’ RadioGraphics, vol. 17, no. 4, July 2010, pp. 851–66. org (Crossref), https://doi.org/10.1148/radiographics.17.4.9225387
- Bajwa, Zahid H., et al. ‘Pain Management in Polycystic Kidney Disease’. Kidney International, vol. 60, no. 5, Nov. 2015, pp. 1631–44. org (Crossref), https://doi.org/10.1046/j.1523-1755.2001.00985.
- Ali, Mohamed Abd Elaziz, et al. “Role of MDCT in Assessment of Inflammatory Renal Disease.” The Egyptian Journal of Hospital Medicine, vol. 69, no. 2, Oct. 2017, pp. 1770–77. org (Crossref), https://doi.org/10.12816/0040602
- Rauschkolb EN, Sandier CM, Patel S, Childs TL. Computed tomography of renal inflammatory disease. Journal of Computer Assisted Tomography. 1982 Jun 1;6(3):502-6 (2012). E g atkinson, mbchb, msc, mrcp. British Journal of Ophthalmology, 75(11), 704–704. https://doi.org/10.1136/bjo.75.11.704-a
- Mahmood, U., Healy, H. G., Kark, A., Cameron, A., Wang, Z., Abeysekera, R., & Hoy, W. E. (2017). Spectrum (Characteristics) of patients with chronic kidney disease (Ckd) with increasing age in a major metropolitan renal service. BMC Nephrology, 18(1), 372. https://doi.org/10.1186/s12882-017-0781-5
- Bansal, V., Lee, J., Kobayashi, L., Doucet, J., Coimbra, R., Fortlage, D., & Reid, C. M. (2014). Determining Injuries from Posterior and Flank Stab Wounds Using Computed Tomography Tractography. The American Surgeon, 80(4), 403–407. https://doi.org/10.1177/000313481408000425
- Rabushka, L. S., & Kuhlman, J. E. (1993). Computed tomography of renal inflammatory disease: Contemporary Diagnostic Radiology, 16(10), 1. https://doi.org/10.1097/00219246-199316100-00001
- Rauschkolb, E. N., Sandier, C. M., Patel, S., & Childs, T. L. (1982). Computed tomography of renal inflammatory disease: Journal of Computer Assisted Tomography, 6(3), 502–506. https://doi.org/10.1097/00004728-198206000-00011
- Piccirillo, M., Rigsby, C., & Rosenfield, A. T. (1987). Contemporary imaging of renal inflammatory disease. Infectious Disease Clinics of North America, 1(4), 927–964. https://doi.org/10.1016/S0891-5520(20)30157-4